
Most coronavirus tests vastly overstate infection, contagion

A recent article in The New York Times has admitted what other researchers have been pointing out online for months: the tests used to detect the newly identified coronavirus are seriously flawed and significantly overstate how many people are infected with quantities of the virus that are likely to cause disease and be contagious, and even overstate how many are still infected at all at the time of the test. In short, the design of the tests produces a significant number of actual false positives and effective false positives.
In order to follow this you have to have at least a basic understanding of how the coronavirus tests work. I'll try to make this as basic as possible; that's the only way I can really understand it myself. Only certain parts of it are really difficult to understand in detail, but those parts aren't critical to catch the point of the article, so I'll simplify them even more.
In case you're unfamiliar with the terminology, "SARS-CoV-2" refers to the particular form of coronavirus that was identified at the start of the outbreak in China late last year as the cause of the new pandemic disease referred to as "COVID-19". It's also important to note at the outset, the test this article discusses is the test widely used all over the world for determining active infection at the time the swab is administered, not the antigen test that looks for antibodies the body produces to fight the virus and indicate only that the virus has been present at some point. A positive antigen test doesn't necessarily mean an individual was infected when the test was performed. A positive virus test is intended to do just that, and likely does if it's designed and performed correctly.
The test used to detect SARS-CoV-2 is based on a process called "RT-PCR", which stands for Reverse Transcription - Polymerase Chain Reaction. The test doesn't look for the virus itself, which is essentially tiny particles of proteins encasing bundles of ribonucleic acid, or RNA (you learned about RNA in Biology class), but instead tests for the presence of the RNA in the material collected from the swab. If RNA in the sequence that has been identified as being from SARS-CoV-2 exists in some quantity in biological material collected with the swab, RT-PCR finds it and determines how much of the virus there is. The quantity of virus detected in the sample is referred to as the "viral load". That's the high-level overview.
Getting a little deeper, the RT-PCR test is essentially a two-step process, but the second step involves dozens of cycles for each single test (I'll explain shortly). The reverse transcription (RT) step takes the single-stranded RNA in the sample and converts it to double-stranded DNA using an enzyme called reverse transcriptase. The resulting DNA is useful because it directly correlates sequentially to the RNA from which it was synthesized but is easier to process for the second step, in part because it's not folded and bundled like RNA.
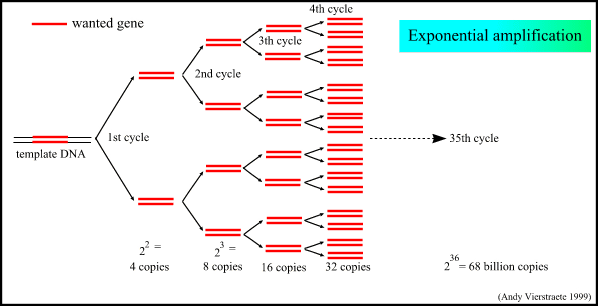
The polymerase chain reaction (PCR) step, which is the most critical step to understand for our purposes, is essentially a DNA manufacturing technique that can take very small quantities of the target DNA (in this case, DNA synthesized from any viral RNA present in the sample) and exponentially increase it so that there's enough of it to be detected and measured. The process starts by splitting (or cleaving) the double-strand DNA into individual strands. Then, complementary strands are grown, again using enzymes, for each of the cleaved strands to create new, intact strands of double-helix DNA in double the amount that was started with. This is essentially the same process that occurs in cell mitosis (cell division).
This process of cleaving and synthesizing strands of DNA is repeated through dozens of cycles of PCR, which produces exponentially more DNA with each cycle, resulting in billions or trillions of strands at the end of the process, depending on how many cycles are performed and how much DNA was present at the outset. If the target DNA isn't there at all due to the person not being infected with the virus, none should be detected, no matter how many cycles are done.
But here's a critical point: if virus is present in the sample but the viral load is low, it takes more cycles of PCR to detect it because there's less target DNA in the PCR process to start with; a high viral load will take fewer cycles to detect it (that's in part how they determine viral load in a PCR test: how many cycles it took to detect the viral DNA). So you would think you would want to do as many cycles as possible to detect the virus to know if someone's infected by it. But it turns out that is not what you want to do, for a very important reason.
Before I explain that reason, there's something else to point out: while the process described above is an accurate, if highly simplified, description of how the test works, when used to diagnose coronavirus infection in each individual, these steps aren't performed in a laboratory setting with scientists in white coats overseeing it, step-by-step for individual-by-individual sample. This testing is carried out by medical personnel not trained in the intricacies of PCR (because they don't need to be) who use test kits prepared by the manufacturer that contain the swab and solution to preserve it in.
The swabs are then processed in the clinic, hospital, or in a testing lab that has a machine that's designed and calibrated to automatically perform the steps described above. The machine performs the number of PCR cycles that the manufacturer has recommended and designed the machine to do. The machine is sort of a "black box" to the technician operating it. They don't necessarily understand how a non-binary test that runs in cycles arrives at a binary "infected/not infected".
If at the end of the specified maximum number of cycles no target DNA has been detected, the machine outputs a negative (there's more information it outputs than that, but that's essentially what it does); if target DNA has been detected at some point before the arbitrary cutoff point in cycles, a positive, or "infected" is indicated.
Each manufacturer sets its own recommended number of cycles of PCR to perform before declaring a negative. If viral DNA is present but the viral load is so low that your cutoff point is below the number of cycles at which the DNA can be detected, then it won't be detected. That sounds like a problem, but it's really not so long as your cutoff point is not excessively low.
And that brings me to a very important reason you don't want to set your PCR cycle cutoff point too high. Setting a cycle cutoff point, or "cycle threshold", too high significantly increases the chances of a false positive result. The reason for that has to do with how the "probe" works. The probe is what detects the existence of, and determines the amount of, target DNA. It's not important to know exactly what it is or how it works, except to say that it has a substance on it that "fluoresces", or glows, when it detects the target DNA. If target DNA is detected, the fluorescence should gradually get brighter with each cycle because double the amount of that DNA is being "manufactured" with each cycle. At any given point, the lighter the fluorescence, the less DNA is present; the brighter, the more.
But the problem with too many cycles is that it can lead to small amounts of DNA -- sometimes very small amounts -- producing fluorescence that it should not have, or at least stronger fluorescence than it otherwise would have. This can make it look like there is more viral DNA there than there actually is, or even make it look like there is DNA of live virus when in fact there is DNA only from inert fragments or debris left over from dead virus, meaning the person isn't infected at all. It does this because too many runs of the cycles can cause background fluorescence to build up on the probe, making it look like a higher load of live viral DNA is being detected when it is not. That can result in a positive test determination when there is very little virus present in the sample, sometimes not even enough to cause illness or contagion, or when there is no virus present at all -- an actual false positive.
How do we know how many cycles is too many? There are a lot of factors that go into it that could cause the correct number to differ. RT-PCR has a number of clinical and research applications beyond being a diagnostic tool for determining viral infection (and the inventor of PCR cautioned against its being used as a diagnostic tool for disease at all), but the academic gold standard for reporting results from PCR is called the MIQE guidelines.
These guidelines were developed by Professor Stephen Bustin after seeing too many studies report RT-PCR results that were not replicable due to insufficient information being reported about the RT-PCR test conditions. The guidelines warn against arbitrary cutoffs as being too high or too low depending on the factors at play, but they state that 40 cycles is the upper end of what should be a reported result from PCR in scientific publications because anything higher is suspect. PCR's creator, Kary Mullis, who won the 1993 Nobel Prize for discovering it, was quoted as saying, "If you have to go more than 40 cycles to amplify a single-copy gene, there is something seriously wrong with your PCR." Others have identified 35 as being the limit beyond which results are questionable and false positives are likely.
Some studies of SARS-CoV-2 have used PCR cycle cut-offs in the mid-30s. At least one, from the European Journal of Clinical Microbiology & Infectious Diseases reported that any sample that required more than 34 cycles to detect virus did not in fact include enough virus to be grown in culture as a benchmark against the RT-PCR. They concluded that any positive based on a cycle cut-off over 34 should not be considered a positive as the patient was not likely ill and was not shedding virus (i.e., was not contagious). They recommended such a patient be discharged and released from any quarantine. (As an aside, part of this study involved significantly shortening the time in which infected patients were cleared using a combination of hydroxychloroquine and azithromycin, confirmed by RT-PCR and cell culturing).
The New York Times' own reporting says that "[t]he C.D.C.’s own calculations suggest that it is extremely difficult to detect any live virus in a sample above a threshold of 33 cycles." So how many cycles do the manufacturers of the RT-PCR tests recommended by the FDA for SARS-CoV-2 in the US recommend as a cut-off? In a review by researcher David Crowe, some of the manufacturers didn't disclose how many cycle were recommended, but among those that did, most of them recommend 40 cycles as a cutoff. A minority of the others recommended cycle cutoffs in the 30s, and two recommended 43 and 45.
Based on those cycle cut-off recommendations, a significant percentage of positive tests could be of people who have so little virus in their systems that they are extremely unlikely to be ill and are not contagious, or they could be people who were not infected at all at the time the swab was administered. This could also be why some people early on in China were found to be testing positive, then negative, then positive again, in as many days.
The New York Times analysis found that "in three sets of testing data that include cycle thresholds, compiled by officials in Massachusetts, New York and Nevada, up to 90 percent of people testing positive carried barely any virus." They went on to say that "[o]n Thursday, the United States recorded 45,604 new coronavirus cases, according to a database maintained by The Times. If the rates of contagiousness in Massachusetts and New York were to apply nationwide, then perhaps only 4,500 of those people may actually need to isolate and submit to contact tracing."
Because I live in Arkansas, a state which has been reported to have had a large increase in positive test cases, I have reached out to the Arkansas Department of Health to find out who manufactures the tests Arkansas uses, whether the tests and manufacturers have changed over time, when they may have changed, and what the cycle threshold or cutoff is for the tests Arkansas uses. As of this writing, I have not received a response. I'll update this article when and if I do.
Some would argue that in a global pandemic tests should err on the side of producing false positives rather than run the risk of missing the presence of virus in an individual, however little virus that may be. But I would argue that a pandemic, with all the fear and irrationality that can come with it, and all the restrains on personal freedom we've seen, is precisely the time when we should be using the most rigorous standards in our testing so as not to add unnecessarily to the fear and paranoia by improperly diagnosing potentially the vast majority of people tested. This is especially true when we're dealing with a virus and a disease that has no unique symptoms that it doesn't share with a number of other diseases and conditions that affect respiration and that are often, though not always, underlying factors to COVID-19. I'm not denying the existence of the virus or that a number of people are getting very sick because of it, including a smaller subset that have no known underlying health conditions.
That being said, an effective false positive is as bad as an actual one. If the NYT is correct that up to 90 percent of those testing positive in the states it analyzed carried barely any virus or none at all, that should be a scandal of the highest degree. If that's true across the country, then the scandal threatens to overwhelm everything we thought we knew about the growth of the pandemic in the United States.
We need to know.
Richie Graham is based in Little Rock Arkansas USA and writes from a free-market libertarian, anti-interventionist perspective.
I should give credit to David Crowe at theinfectiousmyth.com for collecting a significant amount of the information on which this article is based months ago, and starting me on the journey to this research. Although I don't necessarily accept some of his premises and conclusions regarding viruses in general, his documentation of this particular issue with RT-PCR testing was thoroughly researched and footnoted. My article draws significantly, but not exclusively, from his work, and I'm happy and surprised to see his observations being reported in the NYT, even if he's not credited with it.